Chronic pain and opioid usage isn’t new but perhaps our short sighted foray into using long term opioids for moderate to severe pain slowly led to a spiraling of over usage while not recommending adjunct therapies. Several years ago, the Joint Commission of Hospitals listing Pain as the 5th vital sign, which some claim may have inadvertently led to more use of opioids. We now know that chronic opioids are not always helpful for chronic pain and appear to increase astroglial cell activation. We also know that use of opioids in the emergency room and perioperatively at progressively higher doses does appear to lead to “pain ramp up.” However, this does mean narcotics should not be used as they are an essential part of managing severe acute pain.
In the VA populations, there is an exceedingly high use of opioids and nearly half of all opioids prescriptions in the US come from primary care providers. Thankfully the VA population has data miners looking at chronic pain and devices like Biowave are now covered for back pain in the VA setting. Heavy use of narcotics by primary care providers is perhaps not surprising as often they are not widely trained in pain or had training in alternatives to opioids. Plus, in a typical 15-20 minute office visit, writing for an opioid is probably easier than discussing alternatives when someone presents with headaches or back pain.
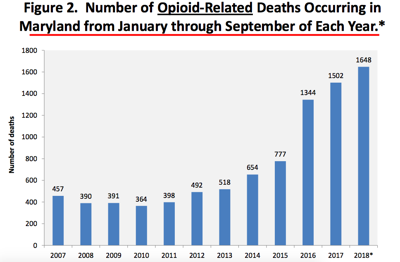
This graph shows we have a real problem in Maryland. The Nationwide map for the US looks similar whether or not deaths from fentanyl are excluded but diversion toward fentanyl is part of the problem
Hospitals, pharmacists, anesthesiologists, and surgeons are seriously exploring whether or not postoperative opioid restrictions will help. Our US federal government recently quickly passed a law that President Trump signed, to explore alternatives and form a task force to curtail the “opioid epidemic.”
One item people are likely too excited about is that Medicare/Medicaid data have shown reduction in opioid prescriptions in States that implemented Medical Cannibas (CBD/THC). However, we still do not know if CBD/THC is a good option for long term pain as several small studies are already suggesting concern. A few studies show that the incidence of nonserious side effects and adverse events is close to 60%, which for most prescription medications would be the end of FDA approval. I’m not saying that Medical Cannibas is all bad as lower ratios of THC and/or pure CBD of the whole plant appears to have several benefits with less incidence of side effects. The unfortunate thing about high dose CBD though is the cost, as monthly administration can get costly.
Good progress is being made with recent Federal White Paper (s) on treatment of pain and pain consortiums looking at alternatives. Thru all this, the field of Integrative Pain Management has been born, which is a field that combines several strategies in pain relief which may include acupuncture, massage, cognitive therapy, neurobiofeedback and biofeedback, electrical forms of pain relief like PEMF, radio frequency/NeuroStim 460, Biowave, photomodulation/Laser/Near Infrared Light, including prescription meds like newer lose dose formulation NSAIDS, Low Dose Naltrexone, nasal and oral ketamine, gabapentenoids, compounded local anesthetics with or without adjuvants like gabapentin, ketamine, plus supplements like oral CBD, CBD ointment, boswella, curcuma, and a few others. Increasingly, we are seeing lower quality evidence (small randomized control trials) therapies move into the moderate quality evidence category due to the increased interest in alternatives.
State and Federal governments are actually looking into Integrative and Alternative medicine to help curtain this problem and have given validity to the field of Integrative Medicine. Even a recent CME course I took for medical licensure had acupuncture and massage as standard of care for back pain. Times are changing.
The good news is that in the last 6 months, we have seen reduction in opioid deaths. Hard to say what is the reason and some suggest having law enforcement carry injectable Narcon may be a large percentage of this. Twice recently, I directly witnessed law enforcement saving 3 lives by using Narcan. One was a situation where I arrived on the scene as a 2 people taking Opioids pulled over on the road and the driver got out and collapsed on the road with respiratory depression with a respirate rate of 2 and constricted pupils and progressing to obtundation. I happened to be driving by and got out to assist. Law enforcement arrived within minutes and injected Narcan. Both individuals immediately were revived to consciousness–when I asked how often they are using Narcan and saving lives, the policemen stated they are now giving Narcan commonly these days.
The bad news in the Opioid World is that in some States, they have a near moratorium on opioid use, and pain clinics around the US and other health care providers are now refusing or simply ran away from writing an opioid prescription. There are a number of chronic pain patients who have been on a stable dose of long term opioids being threatened to have their meds taken away. Let us all remember that for some people, opioids have their place and have given them a higher quality of life. Certainly, some pain clinics running pill mills for profit hasn’t helped the situation, thus why State governments stepped in, but over enforcement of opioid restrictions appears to be a bad thing and careful use of opioids with guidelines is still needed for some people with chronic pain.
We can only hope that task forces understand that States can not just start taking away opioids from those who have been on them long term. We already have a few reports of suicides related to people having their opioid meds restricted.
In the pipeline are a few novel pain medications which may reduce chances of addiction and pain “ramp up” phenomenon that occur with regular opioids and already mixed agonist/antagonist pain meds are helping.
In the meantime, pain clinics like us and others are exploring ways to make IV Ketamine more effective and using this with combination therapy like NeuroStim460, Laser, and powerful PEMF devices to provide greater relief for the very challenging and severe sympathetic pains.
Even more importantly, pain can have an underlying cause. We need to always rule out these causes. For example, I recently had 3 patients come in with daily VAS pain scores above 6-7/10. They were being treated for a “possible rheumatologic condition” and were on NSAIDS and prednisone or methotrexate. Only one of them had a positive ANA or RF autoimmune marker. All 3 happened to have Lyme disease and now they have a VAS score of less than 2/10. 2 of the 3 had a negative Lyme serology thru Labcorp as their primary care provider did entertain Lyme and two did have a history of a Bulls Eye rash, and one had numerous tick bites in the past. The State of Maryland actually has a law that States you will be informed that negative Lyme testing by blood serology does NOT rule out Lyme. Given that Lyme serology has such low sensitivity, many may still have Lyme ! All these patients did display dramatically high TGFB-1 and low MSH on Labcorp testing, consistent with probable Lyme. (mold/CIRS can also cause this) If someone has a knee effusion, migrating pains, fatigue, and occasional headaches, joint fluid should be sent off for Lyme dna pcr as that can often pick it up compared to the low sensitivity of blood serology for Lyme. All 3 patients were on the beginning phases of chronic pain disorder. TGFB-1, MMP-9, MSH hormone all thru Labcorp and a detailed history can be helpful in preventing chronic pain disorder.